 Revision time! CNS and PNS and divisions thereof.
Revision time! CNS and PNS and divisions thereof. Of all the different challenges presented to me in the prehospital environment, I really didn't expect pain management to be something so difficult. We train to resuscitate, to look, listen and feel chests, to palpate abdomens, to stop bleeding; but pain management is so many shades of grey. There are no right or wrong answers if assessment is thorough, but I would argue some assessments and treatments are 'more right' or 'more wrong' than others.
We are taught that pain is subjective and depends on a range of different factors including culture, previous experiences, ability to cope, and that definitive clinical signs cannot be sought as guidance for treatment. Therefore we look to a pertinent history, physical assessment of injuries or patterns of illness and match that up with the available tools in our arsenal and hope that we can make the 'most right' decision.
Pathophysiology of Pain
The pathophysiology of pain is certainly a wormhole...the more you seek to understand the more there is to know! A solid foundation of the nervous system certainly helps (hmm, time for some revision?).
Broadly, pain can be categorised in to Nociceptive and Neuropathic.
Neuropathic pain is complex, chronic pain caused by abnormal processing of stimuli from the peripheral or central nervous system. Nerve fibres can be damaged, dysfunctional or injured, transmitting incorrect signals up the nervous system. An example of neuropathic pain is phantom limb syndrome, where a patient who has had an amputated limb still gets the sensation of the limb, or pain, due to the misfiring of nerves that served the amputated limb.
Causes of neuropathic pain include (but are not limited to); alcoholism, amputation; back, hip or pelvic problems; chemotherapy, diabetes, facial nerve problems (trigeminal neuralgia), immune deficiency, shingles (i.e.: postherpetic neuralgia) and spinal injuries.
Neuropathic pain often presents with shooting, burning pain; or as parasthesia (tingling, pins and needles or similar).
Nociceptive pain, on the other hand, occurs where there is tissue damage—or potential for tissue damage—and can usually be described as sharp, throbbing, aching, cramping etc. This pain can be caused by events such as cancerous growths, trauma, peritoneal irritation, inflammation.
Pathophysiologically it involves four stages: transduction, transmission, perception and modulation. Firstly, tissue damage releases the chemical mediators histamine, prostaglandins, bradykinin, serotonin and substance P (sounds like an early 90's rapper). These substances then activate nociceptors leading to transduction (i.e. propagating and action potential), it's transmitted along the afferent nerve fibres to nociceptors at the spinal cord. It then travels up the spinal cord to the midbrain and thalamus where it is sent to the somatosensory cortex, pariental lobe, frontal lobe and limbic system where perception occurs. Modulation results from activation of the midbrain, multiple neurons in this area release a variety of neurotransmitters that descend to lower areas of the CNS, stimulating the release of more neurotransmitters that eventually lead to the release of endogenous opiates and inhibit transmission of the pain stimulus at the dorsal horn (spinal cord).
Assessing Pain
Prehospitally, everyone knows how much we love (or love to hate...) mnemonics. Thus the OPQRST is used as a way to assess pain, expanded as;
O: Onset
P: Provokation, palliation
Q: Quality
R: Region and radiation
S: Severity
T: Timing
For those with a philosophical bent, the mnemonic SOCRATES may interest you more;
S: Site
O: Onset
C: Character
R: Radiation
A: Associations (signs and syptoms)
T: Timing
E: Exacerbations
S: Severity
For children, the Wong-Baker faces (picture at end of post) was developed to establish pain severity in little people, however its application is quite limited in the prehospital field. In a year or so of working I have found it useful in perhaps three patients; the age it is appropriate for is quite narrow and let's face it, we just don't see that many sick kids.
That being said I was pretty excited when I got to wipe out my Wong-Baker faces diagram for the first time.
Treatment of Pain
Non-pharmacological pain management techniques can't be discounted. While it's easier to give a patient morphine and just get rid of it, reassurance and psychological support has an important role in prehospital pain management. Other injury-specific management (spinning, cold packs, burn aid etc) should also be used in conjunction with pharmacological therapy.
The pharmacological therapy used should be appropriate for the pain expressed. In our kits, we have paracetamol, methoxyflurane, morphine and fentanyl. These are pretty comprehensive in managing acute presentations of pain, but a little more tricky with the chronic pain job.
Understanding the pharmacology of each analgesic your service uses is imperative in making good clinical decisions. Ongoing abdominal pain, ?appendicitis (see previous post), methoxyflurane isn't going to last all that long or assist in this type of pain as much as, say, fractures and dislocations. Extrication of traumatic injuries (limb injuries etc), in particular, can be facilitated much more easily with methoxyflurane as first line agent while gaining IV access and looking towards opiates.
Opiates, on the other hand, act on the central nervous system by binding with opioid receptors and affects the physical and emotional response to pain.
Whatever you choose to use, think about the type of pain and pathophysiology of injury (or suspected injury/illness), the goal of treatment and severity of pain. With good assessment and decision-making the 'most right' answer will be in reach.
Links to more info, and that used in the post, are below:
http://www.medscape.com/viewarticle/735034_2
http://www.ncbi.nlm.nih.gov/pubmed/16774457
http://www.racgp.org.au/afp/2013/march/neuropathic-pain-update/
http://www.jci.org/articles/view/42843
http://www.ncbi.nlm.nih.gov/pubmed/16082232
http://neuroscience.uth.tmc.edu/s2/chapter08.html
We are taught that pain is subjective and depends on a range of different factors including culture, previous experiences, ability to cope, and that definitive clinical signs cannot be sought as guidance for treatment. Therefore we look to a pertinent history, physical assessment of injuries or patterns of illness and match that up with the available tools in our arsenal and hope that we can make the 'most right' decision.
Pathophysiology of Pain
The pathophysiology of pain is certainly a wormhole...the more you seek to understand the more there is to know! A solid foundation of the nervous system certainly helps (hmm, time for some revision?).
Broadly, pain can be categorised in to Nociceptive and Neuropathic.
Neuropathic pain is complex, chronic pain caused by abnormal processing of stimuli from the peripheral or central nervous system. Nerve fibres can be damaged, dysfunctional or injured, transmitting incorrect signals up the nervous system. An example of neuropathic pain is phantom limb syndrome, where a patient who has had an amputated limb still gets the sensation of the limb, or pain, due to the misfiring of nerves that served the amputated limb.
Causes of neuropathic pain include (but are not limited to); alcoholism, amputation; back, hip or pelvic problems; chemotherapy, diabetes, facial nerve problems (trigeminal neuralgia), immune deficiency, shingles (i.e.: postherpetic neuralgia) and spinal injuries.
Neuropathic pain often presents with shooting, burning pain; or as parasthesia (tingling, pins and needles or similar).
Nociceptive pain, on the other hand, occurs where there is tissue damage—or potential for tissue damage—and can usually be described as sharp, throbbing, aching, cramping etc. This pain can be caused by events such as cancerous growths, trauma, peritoneal irritation, inflammation.
Pathophysiologically it involves four stages: transduction, transmission, perception and modulation. Firstly, tissue damage releases the chemical mediators histamine, prostaglandins, bradykinin, serotonin and substance P (sounds like an early 90's rapper). These substances then activate nociceptors leading to transduction (i.e. propagating and action potential), it's transmitted along the afferent nerve fibres to nociceptors at the spinal cord. It then travels up the spinal cord to the midbrain and thalamus where it is sent to the somatosensory cortex, pariental lobe, frontal lobe and limbic system where perception occurs. Modulation results from activation of the midbrain, multiple neurons in this area release a variety of neurotransmitters that descend to lower areas of the CNS, stimulating the release of more neurotransmitters that eventually lead to the release of endogenous opiates and inhibit transmission of the pain stimulus at the dorsal horn (spinal cord).
Assessing Pain
Prehospitally, everyone knows how much we love (or love to hate...) mnemonics. Thus the OPQRST is used as a way to assess pain, expanded as;
O: Onset
P: Provokation, palliation
Q: Quality
R: Region and radiation
S: Severity
T: Timing
For those with a philosophical bent, the mnemonic SOCRATES may interest you more;
S: Site
O: Onset
C: Character
R: Radiation
A: Associations (signs and syptoms)
T: Timing
E: Exacerbations
S: Severity
For children, the Wong-Baker faces (picture at end of post) was developed to establish pain severity in little people, however its application is quite limited in the prehospital field. In a year or so of working I have found it useful in perhaps three patients; the age it is appropriate for is quite narrow and let's face it, we just don't see that many sick kids.
That being said I was pretty excited when I got to wipe out my Wong-Baker faces diagram for the first time.
Treatment of Pain
Non-pharmacological pain management techniques can't be discounted. While it's easier to give a patient morphine and just get rid of it, reassurance and psychological support has an important role in prehospital pain management. Other injury-specific management (spinning, cold packs, burn aid etc) should also be used in conjunction with pharmacological therapy.
The pharmacological therapy used should be appropriate for the pain expressed. In our kits, we have paracetamol, methoxyflurane, morphine and fentanyl. These are pretty comprehensive in managing acute presentations of pain, but a little more tricky with the chronic pain job.
Understanding the pharmacology of each analgesic your service uses is imperative in making good clinical decisions. Ongoing abdominal pain, ?appendicitis (see previous post), methoxyflurane isn't going to last all that long or assist in this type of pain as much as, say, fractures and dislocations. Extrication of traumatic injuries (limb injuries etc), in particular, can be facilitated much more easily with methoxyflurane as first line agent while gaining IV access and looking towards opiates.
Opiates, on the other hand, act on the central nervous system by binding with opioid receptors and affects the physical and emotional response to pain.
Whatever you choose to use, think about the type of pain and pathophysiology of injury (or suspected injury/illness), the goal of treatment and severity of pain. With good assessment and decision-making the 'most right' answer will be in reach.
Links to more info, and that used in the post, are below:
http://www.medscape.com/viewarticle/735034_2
http://www.ncbi.nlm.nih.gov/pubmed/16774457
http://www.racgp.org.au/afp/2013/march/neuropathic-pain-update/
http://www.jci.org/articles/view/42843
http://www.ncbi.nlm.nih.gov/pubmed/16082232
http://neuroscience.uth.tmc.edu/s2/chapter08.html
Identifying neuropathic pain.
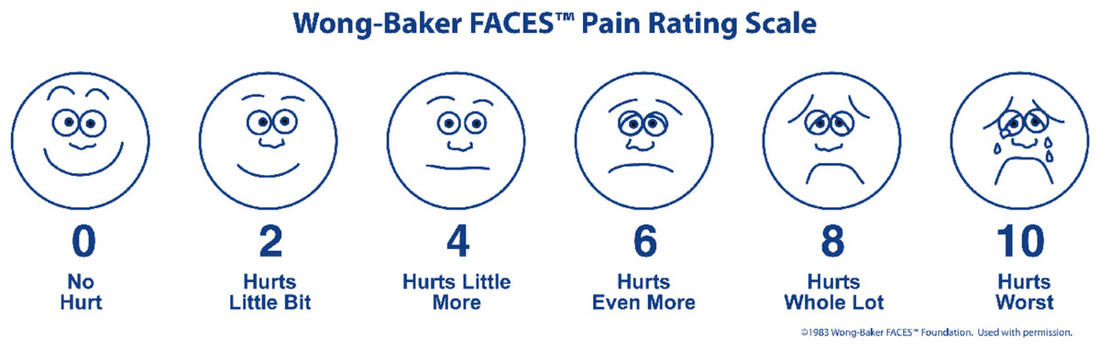
My favourite! Wong-Biker Faces always make me feel '0'.

 RSS Feed
RSS Feed
