
I was going to call this post 'the problem with collars' but shorty after, I was sucked down the literature wormhole and it quickly became apparent that the problem needed to be pluralised.
The fact that the use of hard cervical spine collars for immobilisation in the prehospital is based on premise rather than evidence has been around for a long time. It has been proposed that spinal immobilisation is 'best practice' in the trauma patient with a suspected C-spine injury (CSI) in order to reduce further movement and potential for worsening the existing injury.
Over the past few years there has been more and more evidence that this may not be true.
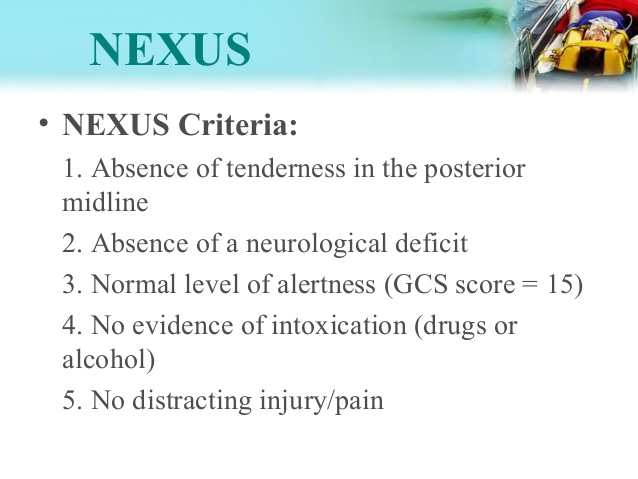
I remember our workshops on KED and NEIJ's: they were paramount to the extrication and spinal immobilisation of trauma patients that may have suffered a spinal injury. With the two major criteria in use: NEXUS and Canadian C-Spine Rule (CCR, see end of post for infographics on both), this means many trauma patients will receive the sentence of a hard collar.
While an extrication jacket, hard collar and spinal board may still be taught as the 'gold standard' for extrication and immobilisation of the trauma patient, out of the OSCE room and workshop it's less common to run the whole gamut of spinal immobilisation. Often the patient involved in an RTC is out of the car, pacing around talking to their insurance company by the time we arrive. Is it really sensible in this case to get them on a spine board to extricate them to the stretcher? In the alert and stable patient it has been found that the incidence of CSI is 1.7%: and surely mechanism, associated injuries or other factors would lead one to identify the patients in which this is a possibility (using NEXUS or CCR).
Yet if the crash he was involved in was at >60km/hr we are directed to collar and immobilise the patient; the mechanism alone is enough for a trauma alert.
While it's postulated that 3-25% of CSI's are secondary, there is no way of proving this to be true due to lack of imaging equipment in the field! It's a long bow to draw to correlate a deteriorating patient in the ward or ED with the care received in hospital/early ED interventions. This data isn't conclusive, is quite antiquated and doesn't control for the fact that at the time this data was made public, broader management of this patient would have looked very different, therefore confounding the results. It's quite likely that in the patient population with worsened outcomes the causal factors would be oedema, haematoma, hypotension, hypoxaemia or inflammation; not likely caused by a piece of plastic around their neck.
Hard collars still remain a standard care in trauma patients, yet there's no reliable evidence for this at all...if anything evidence against routine use of collars is far more forthcoming, including:
—It can compress jugular veins therefore increasing ICP
—Hard collars can force certain population's C-spine into an abnormal position, therefore worsening their outcomes (ankylosing spondylitis)
—Hard collars can make airway management more difficult, is linked to much more difficult intubation, and can make avoiding aspiration in the motion-sickness patient much more difficult
—While they do minimise potential neck movement, 30-degrees of movement is still possible while immobilised; is it possible that a conscious, compliant patient with a possible spinal injury may even be able to manage their C-spine better than hard collars?
—Ill-fitting collars have been linked to poorer outcomes and worsened C-Spine injuries in those with confirmed C-spine injuries
—Using a hard collar along with a spine board has been linked to worsened respiratory status due to 'respiratory restriction' (i.e.: lying on a hard board with a large plastic collar on can make it harder to breathe!).
—Patients in a hard collar are more likely to be subjected to radiological imaging (particularly relevant for children, as there is increasing evidence highlighting the risks of unnecessary imaging in children.
—The full range of spinal immobilisation (hard collar, spine board, blocks and tape) can lead to pressure sores and injuries especially in vulnerable client populations. In the otherwise stable patient with a collar visiting a busy level 1 trauma centre, wait times for CSI clearance can be upward of several hours. If a patient is brought in who is usually immobile, or has injuries that render them immobile henceforth, the time spent on a board can lead to the beginning of (what has been documented as at times fatal) pressure sore development.
Of course, the altered-consciousness patient has an increased risk of CSI, but that doesn't justify the many risks of hard collars as explored above.
Sundstrom et.al's systematic review of the literature surrounding hard collar extrication recommends the omission of hard collars, even in patients with a higher risk of CSI, favouring MILS and spine-board/head block extrication due to the evidence against collars documented above. In certain circumstances collars have been recommended, such as in difficult extrication in RTC's; however it's important to note in this case the collar is recommended as an extrication tool only.
Please check the links below for more information.
Progress in prehospital spinal injury management
http://www.scancrit.com/2013/10/10/cervical-collar/
Why do we put cervical collars on conscious trauma patients?
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2751736/
Pre-hospital spinal immobilisation: an initial consensus statement
http://www.ncbi.nlm.nih.gov/pubmed/24232011
Pre-Hospital use of Cervical Collars in Trauma Patients: a Critical Review
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3949434/
Spinal immobilisation for unconscious patients with multiple injuries
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC515204/
Prevalence of cervical spine injury in trauma
http://www.ncbi.nlm.nih.gov/pubmed/18980470/
The fact that the use of hard cervical spine collars for immobilisation in the prehospital is based on premise rather than evidence has been around for a long time. It has been proposed that spinal immobilisation is 'best practice' in the trauma patient with a suspected C-spine injury (CSI) in order to reduce further movement and potential for worsening the existing injury.
Over the past few years there has been more and more evidence that this may not be true.
I remember our workshops on KED and NEIJ's: they were paramount to the extrication and spinal immobilisation of trauma patients that may have suffered a spinal injury. With the two major criteria in use: NEXUS and Canadian C-Spine Rule (CCR, see end of post for infographics on both), this means many trauma patients will receive the sentence of a hard collar.
While an extrication jacket, hard collar and spinal board may still be taught as the 'gold standard' for extrication and immobilisation of the trauma patient, out of the OSCE room and workshop it's less common to run the whole gamut of spinal immobilisation. Often the patient involved in an RTC is out of the car, pacing around talking to their insurance company by the time we arrive. Is it really sensible in this case to get them on a spine board to extricate them to the stretcher? In the alert and stable patient it has been found that the incidence of CSI is 1.7%: and surely mechanism, associated injuries or other factors would lead one to identify the patients in which this is a possibility (using NEXUS or CCR).
Yet if the crash he was involved in was at >60km/hr we are directed to collar and immobilise the patient; the mechanism alone is enough for a trauma alert.
While it's postulated that 3-25% of CSI's are secondary, there is no way of proving this to be true due to lack of imaging equipment in the field! It's a long bow to draw to correlate a deteriorating patient in the ward or ED with the care received in hospital/early ED interventions. This data isn't conclusive, is quite antiquated and doesn't control for the fact that at the time this data was made public, broader management of this patient would have looked very different, therefore confounding the results. It's quite likely that in the patient population with worsened outcomes the causal factors would be oedema, haematoma, hypotension, hypoxaemia or inflammation; not likely caused by a piece of plastic around their neck.
Hard collars still remain a standard care in trauma patients, yet there's no reliable evidence for this at all...if anything evidence against routine use of collars is far more forthcoming, including:
—It can compress jugular veins therefore increasing ICP
—Hard collars can force certain population's C-spine into an abnormal position, therefore worsening their outcomes (ankylosing spondylitis)
—Hard collars can make airway management more difficult, is linked to much more difficult intubation, and can make avoiding aspiration in the motion-sickness patient much more difficult
—While they do minimise potential neck movement, 30-degrees of movement is still possible while immobilised; is it possible that a conscious, compliant patient with a possible spinal injury may even be able to manage their C-spine better than hard collars?
—Ill-fitting collars have been linked to poorer outcomes and worsened C-Spine injuries in those with confirmed C-spine injuries
—Using a hard collar along with a spine board has been linked to worsened respiratory status due to 'respiratory restriction' (i.e.: lying on a hard board with a large plastic collar on can make it harder to breathe!).
—Patients in a hard collar are more likely to be subjected to radiological imaging (particularly relevant for children, as there is increasing evidence highlighting the risks of unnecessary imaging in children.
—The full range of spinal immobilisation (hard collar, spine board, blocks and tape) can lead to pressure sores and injuries especially in vulnerable client populations. In the otherwise stable patient with a collar visiting a busy level 1 trauma centre, wait times for CSI clearance can be upward of several hours. If a patient is brought in who is usually immobile, or has injuries that render them immobile henceforth, the time spent on a board can lead to the beginning of (what has been documented as at times fatal) pressure sore development.
Of course, the altered-consciousness patient has an increased risk of CSI, but that doesn't justify the many risks of hard collars as explored above.
Sundstrom et.al's systematic review of the literature surrounding hard collar extrication recommends the omission of hard collars, even in patients with a higher risk of CSI, favouring MILS and spine-board/head block extrication due to the evidence against collars documented above. In certain circumstances collars have been recommended, such as in difficult extrication in RTC's; however it's important to note in this case the collar is recommended as an extrication tool only.
Please check the links below for more information.
Progress in prehospital spinal injury management
http://www.scancrit.com/2013/10/10/cervical-collar/
Why do we put cervical collars on conscious trauma patients?
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2751736/
Pre-hospital spinal immobilisation: an initial consensus statement
http://www.ncbi.nlm.nih.gov/pubmed/24232011
Pre-Hospital use of Cervical Collars in Trauma Patients: a Critical Review
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3949434/
Spinal immobilisation for unconscious patients with multiple injuries
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC515204/
Prevalence of cervical spine injury in trauma
http://www.ncbi.nlm.nih.gov/pubmed/18980470/



 RSS Feed
RSS Feed
